


Medicine’s DEI backlash offers an opportunity to build anew
For Nature Medicine, I wrote an essay about the recent backlash over diversity, equity, and inclusion and what comes next, with Dr. Ahmed and Dr. Stone

Diversity, equity and inclusion (DEI) has become a political lightning rod in the USA, with its laudable mission increasingly misinterpreted as a blunt discriminatory tool. Although such critique has been ongoing for decades, it has intensified in academic medicine in recent months, from the resignation of Johns Hopkins’ chief diversity officer over an email on privilege, to efforts within the American Academy of Dermatology to sunset DEI activities. Beyond this pushback, states including Florida, Texas and Alabama have banned DEI efforts in public universities, including their medical schools. Congressman Greg Murphy, a urologist, has recently introduced a bill to cut federal funding for medical schools with DEI policies or requirements.

Press release of Congressman Murphy’s EDUCATE Act to ban DEI in medicine. As DEI advocates, we are concerned about this backlash, but what is more unsettling is how easily DEI has come undone. Although partisan pressure may be a proximal cause, we believe that DEI suffers from an unstable foundation: a poor focus on outcomes and a limited evidence base. We fear that DEI has become a largely performative endeavor that has been unable to diversify the profession or justify its continued need.
Rooted in the Civil Rights Movement, DEI efforts have been ongoing since the 1960s, with its importance in medicine often justified by downstream effects on patient care. For instance, from 1960 to 1964, Black individuals in Jim Crow states had a mortality rate 15% higher than those in non-Jim Crow states, but Medicare’s establishment in 1965 forced hospitals to desegregate, thereby encouraging a more diverse workforce and improving patient outcomes.1 This attention, however, has brought existential challenges, including the first Supreme Court affirmative action case in 1978, after a white man was twice denied admission to the University of California Davis School of Medicine. After more than half a century of DEI efforts and corresponding pushback, it is worth considering: how have these efforts fared?
The data offer a bleak outlook. Between 1997 and 2017, the rate of medical school attendance among members of underrepresented groups fell by 20%, from 4.3 to 3.5 per 100,000 people.2 Similarly, the majority of first-year medical school students have come from the nation’s top income quintile, whereas just 5% came from the lowest.3 Such recruitment failures are mirrored among medical school faculty, with the share of underrepresented minorities among full professors, chairs and deans decreasing between 2000 and 2019.4 The murder of George Floyd in 2020 created public pressure for healthcare institutions to take DEI seriously, so chief diversity officers were rapidly hired and programs were trumpeted out — often with little support. None of these failures are surprising; we were building skyscrapers in a swamp.
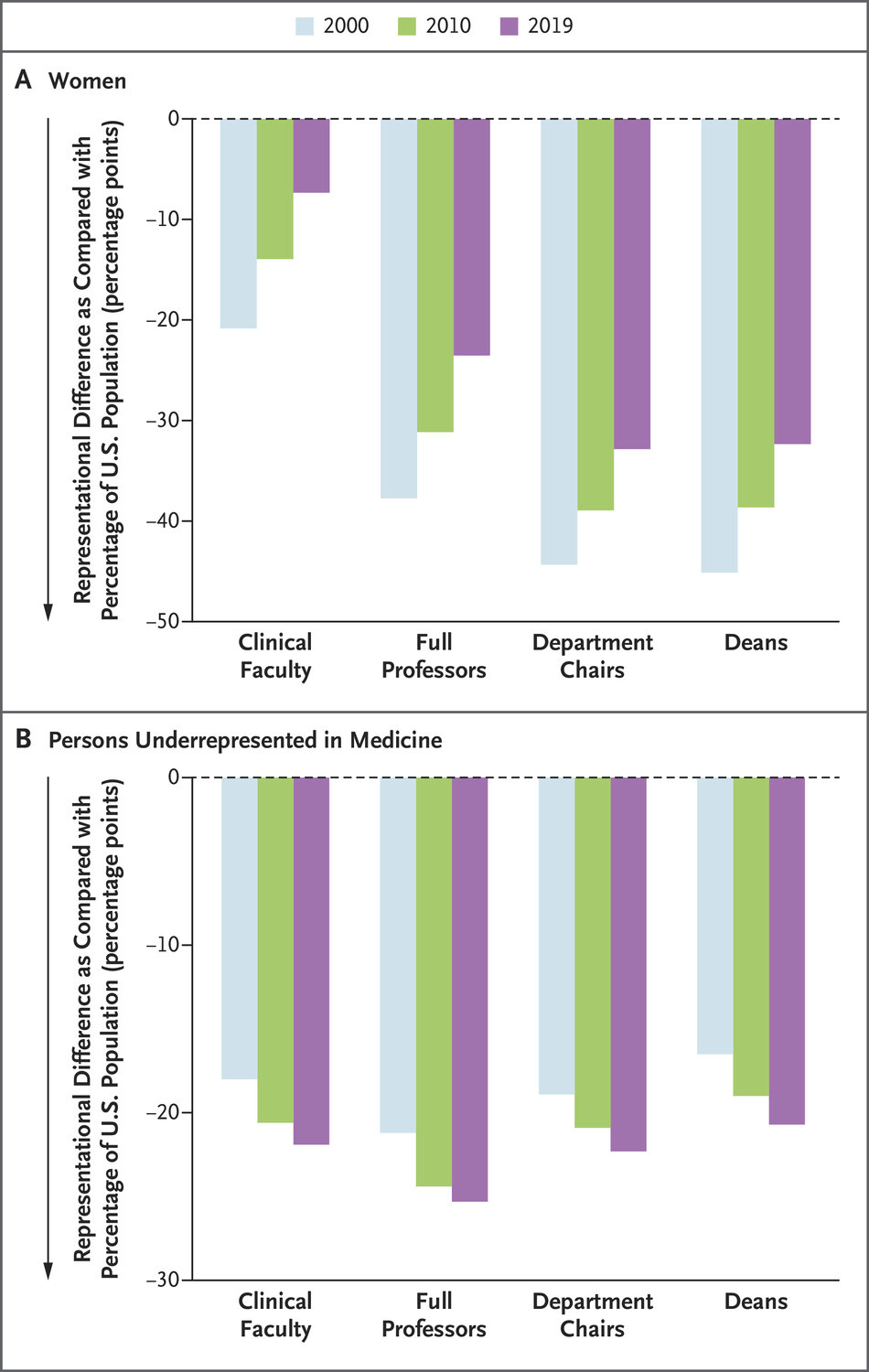
The share of clinical faculty, full professors, department chairs, and deans — relative to the population — has increased from women while decreasing for people underrepresented in medicine from 2000 to 2019 (Sophia Kamran and colleagues for NEJM)We believe that DEI today is hampered by an individualizing myth: that one more implicit bias session, diversity executive, or DEI statement is enough; that with minimal investment, racism can be eliminated from institutions where it is as foundational as their bricks and mortar. Implicit bias interventions, for instance, are commonplace but their enduring effects have not been demonstrated, partly because they are usually one-offs, poorly integrated with broader institutional strategies and unconnected to explicit goals such as improving recruitment.5 Similarly, DEI leaders may become figureheads, tasked with improving the talent pipeline yet unable to change hiring or promotion practices. When public backlash arrives, they are often scapegoated for institutional choices, despite being given limited decision-making authority.6
It is unclear how much money is spent on DEI in medicine, but budgets may be increasing: McKinsey estimates that companies spent US$7.5 billion on DEI-related efforts in 2020, with this sum expected to double by 2026.7 Still, there are limited data to show improved recruitment or the retention of students and staff from minority groups, as well as reduced disparities in care. The goals of DEI cannot be achieved by changing individual hearts and minds, but efforts to prove differently undermine the larger mission and forestall efforts to address more pernicious structural inequities. We are not opposed to DEI, but instead to DEI poorly done, one that fails to provide a return on investment.
What does the alternative look like? We believe it requires real institutional investment, accountability, evidence-based approaches, and a focus on outcomes. First, DEI efforts must start early. The journey to become a physician begins long before opening a medical school application. To recruit and retain underrepresented students in the profession, medical schools and hospitals must proactively address the barriers that they experience, such as a lack of early exposure to health professions, suboptimal science education, and financial hurdles.8,9
Second, with the recent affirmative action case prohibiting the use of race in admissions, DEI initiatives should be recast to focus on socioeconomic status. University of California Davis, for example, has run one of the country’s most diverse medical schools (after the historically Black university Howard and the Hispanic-serving Florida International University) by using class-based affirmative action for the past 17 years.10 Beyond legal reasons, embracing socioeconomic status could offer a ‘big tent’ opportunity for DEI, building greater social support behind initiatives while still achieving racial and ethnic diversification objectives.

Photo of UC Davis medical school’s first class, which was mostly filled with white men. Today, the school is one of the most diverse in the country (Christine Kao for STAT)Third, DEI efforts to enhance recruitment and retention of underrepresented faculty should be implemented at the departmental level, rather than through medical school or hospital DEI offices. At Brigham and Women’s Hospital, for instance, division chiefs at the Department of Medicine set diversity goals using key demographic characteristics and delineate the strategies, receiving financial incentives for their engagement and outcomes. Departments are the recruiting and promoting entities for medical faculty, so basing DEI leadership there is a rational and promising approach. Our institution, Harvard Medical School, has also made DEI a criterion for faculty promotion, which has resulted in broader engagement by providing academic credit for these efforts. This move recognizes the importance of DEI outcomes and eliminates the longstanding assumption that minority faculty alone should be expected to ‘do DEI’ despite being uncompensated and unrecognized (a phenomenon often known as the ‘minority tax’).
Fourth and finally, DEI efforts should be reimagined into an ‘innovation labs’ approach centered on improving healthcare delivery, rather than required one-off sessions and public relations handwringing. Descriptive studies about the poor state of diversity, or associated health outcomes, are already well known and powerless on their own and so should be avoided. Instead, DEI programs that work, such as partnerships between healthcare and public education systems or sponsorship of minority faculty, should be developed, tested and replicated.
With medicine and society appearing to reach a crisis point on DEI, we lament the cynical, partisan campaign to dismantle DEI efforts. However, securing the future of diversity, equity and inclusion in medicine will not come from hastily defending existing efforts, but from acknowledging their failures. This offers the credibility to protect DEI’s underlying mission and build skyscrapers anew with greater clarity. DEI must be made much stronger, more effective, and outcomes focused, and thus be positioned to successfully diversify our profession.
If you’ve made it to the end, I hope it’s because you find these newsletters intriguing and insightful. How can you support work like this? By sharing this newsletter and liking this post. Thanks so much for being here!
Also stay tuned for a post next week on the syphilis epidemic in the United States and what are the most innovative, unconventional ways to address this crisis.